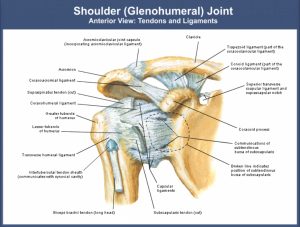
Precautions and Contraindications during Shoulder Rehabilitation following Surgical Intervention.
Shoulder rehabilitation is a complex exercise protocol with the practical application of improved biomechanical and muscle activation guidelines to the repaired anatomic structures in order to achieve the most functional return of the joint. Shoulder
rehabilitation demands the complex return of mobility, control, and speed. Thus, shoulder rehabilitation is a series of controlled exercises starting from the exercises to a stable base of support and muscle activation in trunk and legs to the weaker scapular and shoulder muscles as healing proceeds. This article focuses on some of the important precautions and/or contraindications to be considered during shoulder rehabilitation for the safe and effective outcome.
Precautions/contraindications
- If there is increased pain or irritability in the joint after use of any manual therapy, active, passive or assisted techniques during rehabilitation, it indicates that either the dosage was too strong, the technique is not appropriate or should not be used at this stage.
- The initial and most important priority of shoulder rehabilitation is to address the inflammation around the joint if present. Joint mobilization (Grade III) or stretching techniques are absolutely contraindicated before inflammation subsides.
- Glenohumeral (GH) joint should not be stretched above 90 degrees until there is adequate external rotation range of motion. This is important to prevent suprahumeral impingement.
- Stretching techniques should be gradually progressed until the chronic stage of healing.
- Following a traumatic injury, hypermobile Acromioclavicular (AC) and Sternoclavicular (SC) joints is a common issue. Thus, proper stabilization of scapula and clavicle is important when mobilizing GH joint so as not to stretch AC and SC joints.
- If joint mobilization or gliding technique in the direction of joint restriction is painful or highly irritable, mobilization or gliding should be started in the opposite direction first. Later, as pain subsides, glide in the direction of restriction can be implemented.
- The external rotators and internal rotators of shoulder joint should be strengthened first before dynamic strengthening of abductors and flexors.
- The shoulder is positioned in abduction splint or airplane splint for an extended period (at least six weeks) of time following rotator cuff repair.
- To avoid excessive stress to the anterior capsule and suture line in initial stages of shoulder rehabilitation, passive or assisted shoulder exercises are recommended in the plane of the scapula (Scaption) for patient comfort. During exercises in supine, the humerus is positioned slightly anterior to the midline of the body (by placing the arm on a folded towel).
- Active anti-gravity abduction movement should be avoided following deltoid or supraspinatus repair until the patient can initiate abduction without raising shoulder.
- The patient should be allowed to practice external rotation with the arm at the side only to neutral following subscapularis surgical repair.
- The patient is advised to face the doorway and pulley apparatus while practicing overhead rope-pulley system exercise to improve elevation. This position will limit the shoulder elevation only to a protected range.
- During initial stages of rehabilitation, the patient must avoid weight bearing activities on the extremity, lifting heavy objects and support the arm in a sling during sleeping and extended period of standing or walking.
- In the case of winging of scapula with any resistance or weight bearing exercises, the exercise should be stopped or modified to a lower load bearing. Furthermore, isolated strengthening of serratus anterior, trapezius and rhomboids muscles should be initiated to stabilize scapula in the thorax.
- Shoulder extension exercises are initiated in the prone position from 90 degrees to just short of neutral. Later, is progressed to exercises behind the back.
- Following open repair procedures, dynamic strengthening exercises are only initiated after 3 months and after 8 weeks following mini-open procedures.
- Following open repair patient is advised to avoid functional activities which require overcoming greater resistance force (pushing, pulling, lifting, and carrying heavy loads) for 4 to 12 months postoperatively.
 Until 6 weeks after an open rotator cuff repair, even gentle isometrics are not recommended.
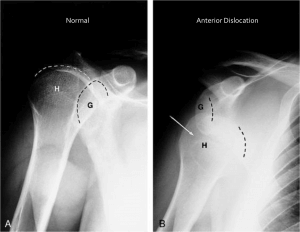
Until 6 weeks after an open rotator cuff repair, even gentle isometrics are not recommended.- Following anterior dislocation of shoulder joint: extension beyond 0 degrees is contraindicated. The forearm is moved from in front of the trunk (maximal internal rotation) to 0 or possibly 10 to 15 degrees external rotation. Also, anterior glide is contraindicated although external rotation is important for a functional elevation of the arm. The shoulder is immobilized in a sling or splint in adduction and internal rotation. The forearm is rested across the abdomen with the arm slightly anterior to the midline of the body.
 Posterior glide is contraindicated following posterior dislocation of the shoulder. The arm is immobilized and supported in an orthosis in the “hand shake” position with neutral rotation, 20-30 degrees of abduction and may be a slight extension of the shoulder).
Posterior glide is contraindicated following posterior dislocation of the shoulder. The arm is immobilized and supported in an orthosis in the “hand shake” position with neutral rotation, 20-30 degrees of abduction and may be a slight extension of the shoulder).
 Until 6 weeks after an open rotator cuff repair, even gentle isometrics are not recommended.
Until 6 weeks after an open rotator cuff repair, even gentle isometrics are not recommended.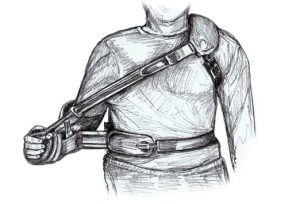 Posterior glide is contraindicated following posterior dislocation of the shoulder. The arm is immobilized and supported in an orthosis in the “hand shake” position with neutral rotation, 20-30 degrees of abduction and may be a slight extension of the shoulder).
Posterior glide is contraindicated following posterior dislocation of the shoulder. The arm is immobilized and supported in an orthosis in the “hand shake” position with neutral rotation, 20-30 degrees of abduction and may be a slight extension of the shoulder).
- Scapular stabilizing muscles are strengthened in an open chain to initiate so as to prevent the weight bearing on an operated upper extremity.
- After an anterior stabilization, internal rotation exercises are contraindicated to initiate from a full external rotation. Similarly, following posterior stabilization, external rotation exercises are contraindicated to initiate from a full internal rotation.

Study on Counter Movement Jump Performance in a Force Platform – Part 2

The A_D_E model of ergonomics practice. A team approach including physiotherapist to workplace safety.

One Comment