Trendelenburg Test – How do you test?
Trendelenberg Test – How do you test it?
Trendelenburg test was first described by Freidrich Trendelenburg in 1895 as a clinical sign to determine the integrity of the function of hip abductor muscles, with specific reference to congenital dislocation of the hip and progressive muscular atrophy. This test is since been used worldwide as a standard method for evaluating hip abductor weakness or as a diagnostic test of function and dysfunction of Hip. However, the details and evaluation method of the procedure is usually described vaguely and have not been standardized. In Apley’s System of orthopedics and fractures, Trendelenburg’s sign as “Normally each leg bears half the body weight. When one leg is lifted the other takes the entire weight. As a result, the trunk has to incline towards the weight-bearing leg. This is achieved by the hip abductors; their insertion is fixed and the pull is exerted on their origin. Consequently, the pelvis tilts, rising on the side not taking the weight. When this mechanism fails Trendelenburg’s sign is positive. The pelvis drops instead of rising on the unsupported side” (Fig. 1). 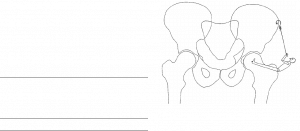
Fig 1. Diagram showing the lever system which acts in the abduction of the hip. (Copied from Vasudevan et al 1997)
Generally, if the patient assumes a one-leg stance and the pelvis drops on the non-test (the non-stance) side, the test result is read as positive; in other words, the hip abductor muscle on the stance side is weak. However, the degree of the knee and hip flexion, trunk lateral sway and moreover the pelvic drop is not immediately obvious and is difficult to report quantitatively. So, in my practice, I still wonder about the most correct way to do a Trendelenburg test. The classical Trendelenburg test was performed as a single leg stance on the test side while non-stance leg side knee is flexed while keeping the thigh extended. Baker et al have reported the false-positive results with this test as the psoas muscle of the non-stance side and abductor muscle of the stance side seem to act in coordination, making difficult even for normal people to elevate the pelvis on the non-stance side without hip flexion on that side.
Hardcastle et al 1985, studied the normal response to the single-leg stance by normal people and also studied the response to the single-leg stance by the people with various abnormalities of the hip and its muscles in order to assess the value and the pitfalls of the classical Trendelenburg test. With this study, Hardcastle et al proposed a Trendelenburg test method which they called the standard Trendelenburg (sT)-test.
Below is the proposed method by Hardcastle et al to do the standard Trendelenburg test:
- The examiner stands behind the patient and observes the angle between the pelvis (the line joining the iliac crests) and the ground.
- The patient is asked to raise from the ground the foot of the side not being tested, holding the hip joint at between neutral and 30 of flexion. The knee should be flexed enough to allow the foot to be clear of the ground in order to nullify the effect of the rectus femoris muscle. The position of the pelvis is again noted. A supporting stick can be used in the hand only on the side of the weight-bearing hip; alternatively. both shoulders can be supported by the examiner so as to maintain balance without a stick.
- Once balanced, the patient is then asked to raise the non-stance side of the pelvis as high as possible. The examiner may support the patient by holding the arm on the stance side.
- If the patient leans too far over to the side of the weight-bearing hip, the examiner corrects this by gentle pressure on the shoulders to bring the vertebra prominence approximately over the centre of the hip joint and the weight-bearing foot.
Interpretation
(a) The response is NORMAL (i.e. the test is “negative”) if the pelvis on the non-stance side can be elevated as high as hip abduction on the stance side will allow, and providing this posture can be maintained for 30 seconds with the vertebra prominens centred over the hip and foot.
(b) The response is ABNORMAL (i.e. the test is “positive”) if this cannot be done. This includes responses where the pelvis is elevated on the non-stance side above the stance side, but where this elevation is not maximal.
(c) The response is also ABNORMAL if the pelvis can be lifted on command, but can not be maintained in that position for 30 seconds. The time taken before the pelvis starts to fall is recorded. By introducing a time element, the Trendelenburg test can be objectively recorded for comparison purposes. Obviously the response described in (b) constitutes a zero time Trendelenburg test.
This method has instructed to elevate the pelvis as high as possible on the non-test side. However, this test does not instruct anything about the trunk sway which we commonly see in our daily practice. So, further study is warranted to determine the effect of trunk sway and hip flexion angle on non-test side in the test result.
Trendelenberg Test – How do you test it? Please comment.

Decorticate and Decerebrate Rigidity. Abnormal Posturing.

Developing Clinical Reasoning
What is the cure or how do you correct?