Achilles tendinopathy (AT) is most common among individuals engaged in recreational or competitive activities. The annual incidence of AT in runners has been reported to be 7% to 9%.
Studies have reported a higher prevalence of Achilles tendinopathy as age increases with the mean age between 30 and 50 years old. The Achilles tendon undergoes both morphological and biomechanical changes. With increased age, Achilles tendon loses collagen diameter and density, glycosaminoglycans, and water content resulting in the reduced elasticity of the tendon. Biomechanically, the aging tendon shows reduced tensile strength, linear stiffness, and ultimate load withstanding capacity.
Cook et al (2009) have proposed to describe the tendinopathy as the tendon continuum. This continuum model has proposed a new strategy to approaching tendon pain staging tendinopathy based on the changes and distribution of disorganization within the tendon.
The three stages are;
Reactive tendinopathy – a stage of inflammatory reaction and edema formation. Failure of treatment or overlooking the tendinitis at this stage may lead to the formation of fibrin and adhesions of the tendon.
Tendon disrepair – if the tendon is not offloaded adequately at the reactive stage there is a continuous production of protein. This increased protein is part of the healing process but with greater involvement may lead to separation of the collagen and disorganization within the cell matrix.
Degenerative tendinopathy – this is the final or chronic stage of the degeneration of the tendon. If the tendon continuum reached this stage, the tendon pain may now have a poor prognosis and degenerative changes are now irreversible.
Improper training activities are a more likely cause of Achilles tendinopathy than the competitive events. Some training errors in runners are cited as a sudden increase in intensity and duration or changes in training surfaces like soft to hard or uphill – downhill or combination of these factors.
Various biomechanical dysfunctions and extrinsic factors like poor training have been largely associated with acute irritation of Achilles tendon. Although there is a paratenon inflammation with acute injury of Achilles tendon, symptomatic Achilles tendon injuries are most commonly associated with the degeneration of the tendon. A degenerated tendon exhibits the signs of neovascularization. This neovascularisation of a tendon is associated with the ingrowths of nerve fascicles which may in part be responsible for the pain associated with Achilles tendinopathy.
Biomechanical dysfunctions:
Abnormal dorsiflexion or subtalar ranges of motion, either decreased or increased, have been associated with Achilles tendinopathy. Kaufman et al. (1999) reported a higher risk of AT by a factor of 3.5 among the athletes with less than 11.5 degrees of dorsiflexion compared to those who exhibited between 11.5 and 15 degrees of dorsiflexion.
McCrory et al. (1999) and Silbernagel et al. (2001) found decreased plantar flexion strength to be associated with Achilles tendinopathy.
Several level 2 studies have reported extrinsic factors like training errors, poor equipment, and environmental factors to be associated with Achilles tendinopathy.
Treatment
Eccentric exercise regimen: many studies have suggested a significant effect of eccentric strengthening program to reduce pain as well as to regain pre-injury functional strength. An eccentric exercise regimen is superior to low energy extracorporeal shock wave therapy (ESWTT); however, the combination of eccentric exercise and ESWTT was better than exercise alone (Silbernagel et al. 2001).
Similarly, modified eccentric loading consisting of unilateral eccentric loading of Achilles without concentric component has shown promising results in the management of Achilles tendinitis. 3 sets of 15 reps, both with the knee extended and flexed, performed twice daily for 12 weeks showed significant outcome (Alfredson et al. 2000).
Stretching regimen: Recent studies have shown poor results with stretching maneuver in terms of both prevention or as an effective intervention for Achilles tendinopathy.
A recent study reported moderate evidence for the use of low-level laser therapy (LLTT) to decrease pain and stiffness in patients with Achilles tendinopathy.
Manual therapy: there is a lack of extensive studies in the effect of manual therapies like joint mobilization, friction massage or soft tissue techniques for Achilles tendinopathy. Some studies have supported the use of joint mobilization in the chronic stage if assessment reveals joint restriction.
Iontophoresis: Carcia et al. (2010), reported moderate evidence for the efficacy of iontophoresis with dexamethasone to decrease pain and improve function in patients with Achilles tendinopathy.
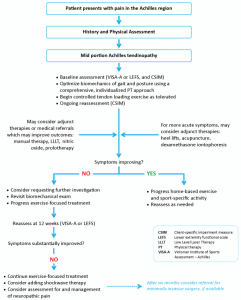
The Achilles Tendinopathy ToolkitThe Achilles Tendinopathy toolkit is an evidence-based clinical decision making aid to assist clinicians in their management of Achilles tendinopathy. (copied from Physiopedia).
References:
Alfredson H, Lorentzon R: Chronic Achilles tendinosis: recommendations for treatment and prevention, Am J Sports Med 29:135- 46, 2000.
Carcia CR, Matin RL, Houck J, et al. Achilles pain, stiffness, and muscle power deficits: Achilles Tendinitis Clinical Practice Guidelines, JOSPT 40(9): A1 – A26, 2010.
Mc Crory JL, Martin DF, Lowery RB et al: : Etiologic factors associated with Achilles tendinitis in runners, Med Sci Sports Exerc 31: 1374 – 81, 1999.
Silbernagel KG, Thomee P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain – a randomized controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports 11: 197 – 2006, 2001.
BC Physical Therapy Tendinopathy Task Force: Dr. Joseph Anthony, Allison Ezzat, Diana Hughes, JR Justesen, Dr. Alex Scott, Michael Yates, Alison Hoens. Achilles Tendinopathy Toolkit. A Physical Therapy Knowledge Broker project supported by: UBC Department of Physical Therapy, Physiotherapy Associaton of BC, Vancouver Coastal Research Institute and Providence Healthcare Research Institute. 2012 (Level of Evidence 5).